- home
- Facial plastic surgery
- Plastic surgery, midface lift - indications and techniques
Facial aging depends on several factors: heredity, lifestyle (sleep, sun, cigarettes), self-care, general health, and also, to a large extent, weight stability. It is impossible to clearly determine when a patient will need facial plastic surgery. It makes no sense to focus on age in this matter, since the basis for the operation is objective medical indications and individual aesthetic requirements.
Diagnosis and aesthetics of age-related changes in the midface
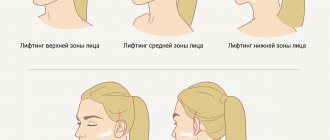
First of all, age-related changes become noticeable in the upper and middle third of the face. While the lines and wrinkles that bother a patient in the first place are not that difficult to correct, they are almost never significant to the overall architecture of the face. The midface (the area between the lower eyelid and the mouth) is very important for aesthetic perception. More clearly than any other aspect, a person’s youth and health are revealed not by the presence or absence of wrinkles, but by the shape of his face. The beautiful and young central part has a pronounced volume in the cheekbones, rounded shapes and is distinguished by a smooth transition between the lower eyelid and the cheekbone; the nasolabial fold is soft, not pronounced. Due to the sufficient volume of this zone, a young face has the shape of an inverted cone. With age, this facial architecture changes completely - the cheeks become flat, losing volume and shape on top. At the same time, the lower part accumulates fat, the skin sags, the lines of the nasolabial fold are distorted, voids and excess skin form under the eyes.
Contraindications and restrictions
All of the listed methods for lifting the middle third of the face are gentle - they do not require special preparation or long-term rehabilitation. You can return to your normal life immediately after the lifting (although bruising and swelling still occur). Despite this, there are a number of limitations. Injections and threads should not be given to people who:
- there are blood clotting disorders;
- pregnancy and lactation;
- there are severe chronic diseases, including endocrine ones (for example, diabetes mellitus);
- there are inflammations, rashes, wounds at the treatment site;
- an infectious disease is determined in the acute phase.
For women, injections are not recommended in the first half of the cycle - at this time the walls of the blood vessels become more susceptible, and bruising is more likely.
To make an appointment for facial correction with fillers in Moscow, call us or fill out the form on the website. Clinic “BL” is located within walking distance from the Oktyabrskoye Pole metro station, our address: st. Marshala Rybalko, 2k6. Our experienced specialists will select the optimal method for your case and help you restore your skin to a fresh and radiant look.
Criteria for assessing age-related changes in the midface
The modern concept of plastic surgery considers the face as a single whole. In particular, the lower eyelids and cheeks are included in the middle zone complex. Therefore, the processes occurring in it must be analyzed precisely in this context in order to obtain a good rejuvenating effect. The middle zone of the face consists of the lower eyelids, cheek and zygomatic areas. As a rule, changes in all these parts of the face are interconnected. To analyze the midface area we consider:
- lower eyelids
the presence of excess skin volumetric changes, the presence of a tear trough the size of the palpebral fissure the position of the lateral angle of the eye the height of the lower eyelid the transition of the eyelid-cheek, eyelid-cheekbone
- volumetric changes in the cheeks and cheekbones
- presence of ptosis or excess skin in this area
- depth of the nasolabial groove
Age-related changes in the midface
With age, the proportions of the face change, the volume from the upper and middle parts of the face moves down, the malar fat, located at a young age above the cheekbone, slides down, causing deformation not only of the cheek, but also of nearby tissues. In this regard, the main task of the surgeon when reconstructing the midface is to move the volume upward, create a high line of cheekbones with sufficient roundness and volume, reduce the length of the lower eyelid, soften the severity of the nasolabial fold, and straighten the tear trough.
Age-related deformation of the midface is caused by many factors: the structure of the skin, subcutaneous tissue and facial skeleton, relaxation of the supporting connective tissue ligaments and others. Correcting this zone requires special knowledge and skills, taking into account a lot of factors.
The thickness of the tissue varies significantly in the midface. Due to the difference in their anatomical structure, the use of drugs with different viscoelastic properties is required. Drug administration levels also vary from zone to zone.
An important factor in the formation of the bucco-zygomatic and palpebromalar grooves is bone atrophy and/or hypoplasia of the upper jaw and zygomatic bone, which affects the condition of the overlying tissues even in the middle age group. Therefore, to compensate for the volume deficit of bone structures (zygomatic bone), especially in patients with deformation morphotype of aging, it is advisable to use a drug with good supporting ability (Restylane SubQ), which will give the maximum lifting effect.
The tip of the nose and the tear trough are considered the highest risk areas for correction.
Contour injection plastic surgery of the zygomatic area
This type of correction involves replenishing the volume of the zygomatic region (especially with underdevelopment of the zygomatic bone) and indirectly reducing the palpebromal and nasozygomatic grooves. The recommended technique is a fan, 0.1 – 0.4 ml (per vector), bonewise, the volume of injected high-viscosity drug is 1.0 ml per side.
Contour injection plastic of the palpebromalar groove
This type of correction along the lower anterior edge of the orbit is carried out to eliminate the deficit in tissue volume in the periorbital region. The correction is carried out using pinpoint injections (multipuncture) or a fan, in small portions (0.05 ml each), bonewise along the anterior (facial) surface of the processus zygomaticus os maxillae and margo infraorbitalis os zygomaticum under m. orbicularis oculi (into the layer of axillary fatty tissue, preventing the introduction of material into the orbital area). For correction, a medium and high viscosity gel based on HA is used, for example, Restylane or Restylane Perlane (depending on the thickness of the integumentary tissue), in a volume of no more than 0.5 ml on one side.
Contour injection correction of the cheek-zygomatic groove
This manipulation consists of increasing the volume of soft tissue in its projection and maximizing stabilization of the area due to the so-called stitching of tissue.
A linear technique is used to administer the drug perpendicular to the surface of the skin through all skin layers and the layer of subcutaneous fat (avoiding injury to the a., v., n. infraorbitalis and a., v., angularis). For correction, 0.5 to 1.0 ml of HA gel is used (less viscous for thin skin, for example, Restylane). With an unexpressed nasozygomatic groove, a uniform linear “stitching” (filling) is sufficient, whereas with a pronounced deficiency (depression) of tissue in this area, it is necessary to additionally create a volume in the form of a pyramid (base down) or a drop due to a greater introduction of the drug into the subcutaneous fat layer .
Depending on the severity of the deformity, age and wishes of the patient, a combination of all three types of correction or their separate combination is possible.
Possible vascular complications
The blood supply to the soft tissues of the face is carried out to a greater extent from the external carotid artery and to a lesser extent from the internal one. Venous outflow occurs through a system of veins that flow into the facial and mandibular veins (v. retromandibularis), and from there into the internal jugular vein (v. jugularis interna).
In addition, the facial vein system has a connection through the external ophthalmic vein with the intracranial cavernous sinus, which theoretically creates the risk of severe complications when the injected material spreads along the venous tract.
According to one or more criteria, potentially dangerous anatomical areas include the cheek-zygomatic zone and the area of the nasolabial fold (its upper part). Vascular complications in the area of the middle third of the face occur during correction of the tear trough, nasozygomatic groove, nasolabial folds, and volumetric plastic surgery of the middle zone of the face. In these cases, embolism (compression) of the facial artery and vein (a., v. facialis) and infraorbital vessels (a., v. infraorbitalis) is possible. The facial artery and veins emerge most superficially (under the platysma) in the projection of the anteroinferior edge of the masticatory muscle (bending over the edge of the lower jaw) and at the base of the nasal wing, where the artery and vein are located in the subcutaneous fat. In other parts of the face, these vessels pass in the deep layer of fatty tissue between the facial muscles.
To replenish the volume of fatty tissue, depending on the thickness of the integumentary tissue, drugs with a greater degree of integration into the tissue are used, namely: Restylane - in the periorbital area, Restylane Perlane - in the cheek area.
The infraorbital neurovascular bundle comes to the surface through the infraorbital foramen (0.5 - 1.0 cm below the line of articulation of the zygomatic bone and the upper jaw). When performing deep injections in this area, trauma to both blood vessels and the sensory nerve is possible.
The blood supply to the tissues of the external nose comes mainly from the system of the external and internal carotid arteries: the angular artery (a. angularis) is a branch of the anterior facial artery (a. facialis anterior), the dorsal nasal artery (a. dorsalis nasi) is the terminal branch of the orbital artery (a . ophthalmica), originating from the internal carotid artery system. The branches of the corresponding paired arteries anastomose with each other at the level of the dorsum of the nose. The blood supply to the tip of the nose comes from several sources: the arteries descending the dorsum of the nose, the lateral nasal artery and the artery of the upper lip. These thin vessels are subject to compression with the subsequent development of ischemia when filler is injected excessively.
Despite knowledge of the anatomy of the vessels, when injecting fillers in dangerous anatomical areas, one should adhere to the recommendations for the injection technique (slow injection and aspiration test), and if symptoms of drug embolism or compression occur, immediate active therapy should be started.
Author: Elena Karpova, Doctor of Medical Sciences, Professor, Associate Professor of the Department of Skin Diseases and Cosmetology, Russian National Research Medical University named after. N.I. Pirogova, Moscow.
Magazine: Appearance. Esthetic guide №3(20)
Indications for midface plastic surgery
If you have drooping and sagging tissue in the cheek area, deep tear troughs are visible, the lower eyelid has lengthened (vertically), the contours of the cheekbones have been smoothed - then a midface lift is an operation that will correct all these shortcomings. Obvious indications for a midface lift are pronounced protrusions of fat under the eyes, lacrimal, eyelid-buccal, zygomatic grooves, “malar” or zygomatic “bags”. Midface lift is also used as a corrective operation for rounding of the eyes, in patients who have previously undergone traditional blepharoplasty on the lower eyelids, with slight inversion of the lower eyelid, in patients with “recession” of the lower eyelids.
Preparations for facial contouring
Injectable preparations differ in the concentration of the active substance, density and viscosity. Those with the densest structure are more suitable for facial volumization and complex procedures. Preparations with a lighter structure are intended for filling folds, skin creases, and furrows. Taking into account the main component, the following types of fillers are distinguished:
- based on hyaluronic acid
are the most common preparations on the cosmetic market. This acid is produced by the body, so the drugs are safe and do not cause allergic reactions. They give a harmonious and attractive correction result. In addition to volumization, they provide intense hydration; - based on potassium hydroxyapatite
- just like hyaluronic acid, it is present in the body as part of bone tissue. The preparations model a clear, beautiful oval of the face and achieve lasting lifting; - based on polycaprylactone
– a relatively new group of drugs. It is based on a substance used in surgery as an absorbable suture material. The peculiarity is the long-term preservation of the correction result.
There are many different fillers. The most popular preparations based on hyaluronic acid, for example, from the company Galdema, include Restylane, Restylane perlane and Allergan - Juviderm. One of the preparations based on potassium hydroxyopatite is Radiesse.
. This is a powerful collagen stimulator, which is used as a volumizer to create additional volume and shape. The choice of filler for a particular area should only be made by a doctor with the necessary knowledge and skills.
Frequently asked questions during facial plastic surgery
1. Indications for facial plastic surgery Indications for facial plastic surgery are: drooping soft tissues of the face, excess skin in the upper and lower thirds, wrinkles in the face and neck area.
2. Anesthesia
The operation is performed only under general anesthesia with the addition of local anesthesia.
3. Where will the incisions be, will scars be visible?
The standard incision for a face and neck lift begins in the scalp of the temporal region, disappears into the auricle, going around the lobe, where it ends. Intradermal sutures are placed on the wound of open skin areas, which subsequently makes the scars invisible.
4. Duration of operation
The operation lasts from 1.5 to 2 hours
5. How many days to stay in the clinic after surgery
After the operation, you must stay in the hospital for the first day or two. In the first hours, ice should be applied to the intervention site to reduce postoperative swelling and the likelihood of bruising.
Methods for correcting the midface area
There are several ways to correct the situation and restore the required volume in the upper cheek and lower eyelid area. They are distinguished by the degree of complexity and traumaticity of the procedure, rehabilitation time, cost, as well as the degree of severity of the result.
Cheek lift
The goal of midface plastic surgery is harmonious rejuvenation of the entire periorbital region and midface. It allows you to restore the “youthful” contour of the entire face, which is sometimes not achieved with a regular traditional facelift. Subperiosteal correction of the midface can be performed simultaneously with other anti-aging facial surgeries - lifting the lower third of the face and neck, installing facial implants and lipofilling. Often cheek lift is combined with lower eyelid plastic surgery; in this case, there is only one seam, since the tightening of the skin and muscles of the middle zone of the face is carried out through an incision under the ciliary edge of the lower eyelid. Sometimes, in the absence of excess skin, the operation can be performed transconjunctivally - through an internal incision in the lower eyelid. Another method of correction is an incision in the temporal part of the head. In fact, we can consider that rejuvenation of the midface is a whole complex of operations associated not only with the elimination of sagging skin, but also with the upward displacement of the muscle complex of the cheek. To secure tissue during such an operation, it is effective to use endontins - special fixatives that dissolve over time, leaving the tissues fused in the correct position.
Another method of performing this operation is endoscopic midface lift. In this case, access is carried out through an incision inside the mouth; there are no external incisions left after the operation; the progress of the operation is monitored through a special device that allows you to monitor the progress of the operation on the monitor screen. The difference in the methods of performing the operation lies not only in the access, but also in the direction of tissue tightening. In the case of access through the lower eyelid, we obtain a strictly vertical lift of the middle zone; with temporal and oral access, the tissues are pulled diagonally upward. The presence of excess skin is also important for choosing a correction method. Diagnostics in this case allows you to choose the best method for a particular patient. Other methods for correcting age-related changes in the midface
Alternative correction of the midface using the lipofilling method
The peculiarity and main direction of development of modern aesthetic surgery is the search for the least invasive and traumatic methods of appearance correction. And today, it is possible to achieve significant results when reconstructing the midface using less invasive methods. These include thread lifting and lipofilling. Lipofilling - the introduction of the patient’s own fat into the corrected areas, allows not only to create volume, but also to imitate the necessary shape, smooth out unevenness and has an extremely beneficial effect on the skin, significantly rejuvenating it due to the presence of a large number of growth factors in the fat.
Conclusion: sometimes during diagnosis it is obvious that it is inappropriate to carry out a full cheek lift. In such cases, lipofilling allows you to solve problems in a much less traumatic way with equal aesthetic results. Of course, the decision on correction methods is made after careful consultation between the surgeon and the patient. Regardless of the chosen correction method, the result of reconstruction of the middle zone of the face will be a changed contour of the cheek, the disappearance of the tear trough, and smoothing of the nasolabial folds.
Temporal lifting
Temporal lifting is another modern method of endoscopic lifting of the midface. When performing such plastic surgery, incisions are made in the temporal part of the head, laterally (inside the mouth) and along the lower eyelid. Until recently, the main disadvantage of temporal lifting was the inability to adequately correct ptosis of the cheek tissue. The result was not entirely natural due to the point fixation and incomplete coincidence of the vector of tissue movement (from below diagonally, towards the temple, and not exactly against the direction of age-related ptosis, which always moves tissue from top to bottom). The temporal lifting technique was reborn with the development of endotins. Their use made it possible to achieve the main effect - to obtain a harmonious and natural result when lifting the cheeks.
Compared to a check-lift, this operation is more invasive. Its duration is about 2 hours. The recovery period is also longer – 3-4 weeks. For several months after surgery, endotins, which fix the tissue, can be felt under the skin. Then the tightened tissues take root in their new position, and the endotins are completely absorbed.