Causes of diastasis after childbirth and provoking factors
The abdominal wall consists of supporting and connecting tissue, including collagen fibers. Due to pregnancy hormones, the tension in the fibers decreases and they begin to stretch, and the abdominal muscles give way to the growing baby. The separation of the rectus abdominis muscles along the midline of the connective tissue connecting them (linea alba) is called diastasis. The linea alba runs from the bottom of the sternum to the top of the pubis and is usually about 1 cm wide. Diastasis can occur anywhere from the top to the bottom of the midline. After delivery, this process will resolve itself and the collagen fibers will regain their normal traction force. However, prolonged stretching or tearing of the fibers may cause the binding tissue to fail to fully repair itself.
Having diastasis is completely normal during the third trimester. However, there are a number of factors that can increase the likelihood of developing a disorder that will be difficult to correct:
- Pregnancy after 35 years
- Already have two or more children
- C-section
- Pregnancy with twins or triplets
- Large baby or increased amount of amniotic fluid
- Incorrect type of load on linea alba during pregnancy
- Constant constipation
- The wrong kind of strength training during or after pregnancy
Diastasis of the rectus abdominis muscles
What is diastasis recti?
The rectus abdominis muscles are separated by a dense connective tissue septum - the linea alba, formed by tendon stretches of the oblique and transverse abdominal muscles on both sides. Normally, the inner edges of the rectus abdominis muscles are quite tightly adjacent to each other, and the width of the white line usually does not exceed 1 - 2 cm. Diastasis of the rectus abdominis muscles is a divergence of the rectus abdominis muscles, an increase in the width of the white line by more than 2 cm.
Is diastasis recti a hernia?
Diastasis of the rectus abdominis muscles is not a classic abdominal hernia, since it does not have a hernial orifice and there is no risk of strangulation of internal organs. But traditionally, diastasis of the rectus abdominis muscles is considered within the framework of herniology (a surgical discipline that studies abdominal hernias), since the principles of reconstruction of the anterior abdominal wall and abdominal hernias are similar. In addition, diastasis of the rectus abdominis muscles is often combined with hernias of the white line and umbilical hernias.
Who gets diastasis recti?
Diastasis of the rectus abdominis muscles is more common in middle-aged or older men with abdominal (central) obesity and in slender women after pregnancy. Moreover, in men, diastasis of the rectus muscles most often occurs in the epigastric region (upper abdomen), and in women - in the mesogastrium and hypogastrium (in the middle and lower abdomen).
Why does diastasis of the rectus abdominis occur?
The main causes of diastasis of the rectus abdominis muscles are congenital weakness of connective tissue (connective tissue dysplasia) and stretching of the linea alba as a result of increased intra-abdominal pressure or mechanical load. If for men the risk factors are heavy physical activity and obesity, then the main risk factor for diastasis of the rectus abdominis muscles in women is pregnancy and childbirth. During pregnancy, significant stretching of the anterior abdominal wall and the white line occurs. In addition, during pregnancy, as a result of hormonal changes, softening and stretching of the ligaments occurs. Additional risk factors are pregnancy with a large fetus, polyhydramnios, multiple pregnancies, and repeat pregnancies.
What kind of diastasis of the rectus muscles occurs?
Depending on the severity of the expansion of the white line of the abdomen, 3 degrees of diastasis of the rectus abdominis muscles are distinguished: I degree - the width of the white line is up to 5 - 7 cm, II degree - the width of the white line is more than 5 - 7 cm, III degree - a combination of diastasis of the rectus muscles with a saggy abdomen .
In plastic surgery, another classification of diastasis of the rectus abdominis muscles is used:
- A – diastasis of the rectus abdominis muscles in women after pregnancy and childbirth
- B – diastasis of the rectus abdominis muscles in combination with “relaxation” of the lateral abdomen and lower part of the anterior abdominal wall
- C – diastasis of the rectus abdominis muscles, extending in the epigastrium to the xiphoid process and costal arches
- D – diastasis of the rectus abdominis muscles in combination with the absence of a waist
The most common type A diastasis of the rectus abdominis muscles occurs, that is, in women after pregnancy and childbirth.
How does diastasis of the rectus abdominis muscles manifest?
A small diastasis of the rectus abdominis muscles usually does not cause any complaints, except for the presence of a protrusion in the midline of the abdomen, which appears during physical activity and disappears with rest. With large diastasis, discomfort and abdominal pain may periodically occur. But in general, diastasis recti is an aesthetic problem, and most operations are performed for cosmetic reasons. If diastasis of the rectus abdominis muscles is combined with a hernia of the white line of the abdomen or an umbilical hernia, then surgical treatment is indicated as planned, for the same indications as for other hernias.
What examination is necessary for diastasis of the rectus abdominis muscles?
To diagnose diastasis of the rectus abdominis muscles, an examination of the patient is usually sufficient. If you try to raise your head and upper half of your body while lying down, a characteristic keel-shaped protrusion will appear in the midline of the abdomen, disappearing with rest. In cases of severe diastasis of the rectus abdominis muscles and its combination with hernias, it may be advisable to perform an ultrasound examination of the anterior abdominal wall (US) or computed tomography (CT) of the abdominal cavity. These studies provide accurate information about the distance between the rectus abdominis muscles, the size of the hernial orifice in the presence of an umbilical hernia or white line hernia, the nature of the hernial contents, and allows one to calculate the volume of the hernial sac and the volume of the abdominal cavity. This data is extremely necessary for choosing an operation. All patients with diastasis of the rectus abdominis muscles must undergo an ultrasound examination of the abdominal cavity and pelvis before a planned operation, so as not to miss the presence of other pathology of the abdominal organs.
What are the treatment tactics for diastasis of the rectus abdominis muscles?
In most cases, the indications for surgical treatment of diastasis recti are cosmetic. But with grade III diastasis, accompanied by complaints, limitation of physical activity, combined with hernias, there are absolute indications for planned surgical treatment.
In women after childbirth at the initial stage of the disease, diastasis of the rectus abdominis muscles can be corrected with the help of special physical exercises. However, if conservative treatment does not bring any effect or there is diastasis of II – III degree, combined with abdominal hernias, surgical treatment is performed.
Considering that the indications for surgical treatment of diastasis are often cosmetic in nature, preference is given to minimally invasive surgical operations. Most often, a small semilunar skin incision is made in the navel area or a transverse incision up to 6–7 cm along the skin fold above the pubis. If there is a scar after a cesarean section, it is usually used for surgical correction of diastasis. Using special elongated instruments, subcutaneous fat is separated from the linea alba of the abdomen throughout this diastasis (if necessary, from the costal arches to the pubis). Then, using a continuous suture using long-absorbable suture material, the separated inner edges of the rectus abdominis muscles are sutured. Thus, the linea alba is reconstructed and diastasis of the rectus abdominis muscles is eliminated. If necessary, a synthetic mesh implant is additionally used, which further strengthens the suture line. In some cases, it is possible to use endoscopic support to fix a synthetic implant to the anterior abdominal wall from the abdominal cavity.
In the presence of overstretched skin with striae (stretch marks) in the lower abdomen, it is advisable to combine correction of diastasis with abdominoplasty. This is a surgical intervention in which excess overstretched skin and subcutaneous fat are removed, and the waist and contours of the abdominal wall are formed.
Symptoms and methods for determining the presence of diastasis
Diastasis after childbirth is not accompanied by any pronounced clinical symptoms, but can cause the following unpleasant disorders:
- Problems with posture and increased stress on the spine
- Also, diastasis after childbirth can be complicated by the appearance of a hernia.
How to determine diastasis after childbirth? To identify such changes, you can resort to a simple test at home:
- Lie on a hard surface, such as the floor, bend your knees and place your feet on the surface.
- One hand should be placed behind the head and the other on the stomach, gently touching the midline of the abdomen with your fingers (the line is parallel to the waist, in the navel area).
- Next, you need to take a deep breath and exhale, relax the abdominal cavity and press on it with your fingertips.
- Then you should raise your torso and fix yourself in this position for a few seconds. During this time, you can feel how many fingers fit between the abdominal muscles and determine the “space”.
Such self-diagnosis will allow us to identify the size of the “space” and at least approximately know the degree of discrepancy. The more fingers the “space” has absorbed, the more pronounced the diastasis.
If you find such a “gap” a few weeks after giving birth, there is no need to panic. Over time, the connective tissue will return to normal and elasticity will resume. However, do not forget about special exercises that will speed up the recovery process.
Diastasis usually recovers naturally within the first six months after childbirth. After pregnancy, you can check your diastasis monthly to monitor your progress.
Diastasis of the rectus abdominis muscles - symptoms and treatment
Diastasis of the rectus abdominis muscles does not always require surgical correction. For women who are less than 12 months postpartum and overweight patients who have not previously tried to correct diastasis with exercises, it is recommended:
- control weight: body mass index (BMI) should not exceed 26 with an average build;
- do exercises to strengthen the anterior abdominal wall [1][8].
Exercises for diastasis
There is no single set of exercises; different trainers use different programs. It should be noted that all exercises are aimed at strengthening the muscular frame of the abdominal wall, but they do not always help reduce the width of the white line of the abdomen [8][10]. For diastasis, it is recommended to perform the following exercises:
- Supination (outward rotation) of the knee in a position on all fours . Starting position - emphasis on your knees and straightened arms. From this position, bend your left leg and bring your knee towards your sternum, then do the same with your right leg. You can perform 10 repetitions on each leg, 5-6 approaches per day.
- Exercise " plank " and its variations. The emphasis can be placed on your knees or toes, on your elbows or straightened arms. This is a static exercise; it does not lead to excessive muscle stretching. The execution time gradually increases from 20 seconds to 1 minute. Perform 3–5 approaches per day.
- Exercise "to the eye " . In a position on all fours, as you exhale, arch your back upward, rounding it like a cat, while straining and drawing in your stomach as much as possible. Keeping your muscles tense, exhale and slightly bend your back in the opposite direction. Do 10–15 repetitions, 3–4 sets per day.
- A set of Kegel exercises. They are aimed at strengthening the abdominal and pelvic floor muscles. Technically, these exercises are not difficult, but they must be performed carefully. If the technique is incorrect, the effect can be the opposite. It is recommended to do approaches 3-4 times a day for 10-15 minutes. As a rule, the effect appears after 4–6 weeks.
Classic exercises for strengthening the abdominal muscles with lifting and twisting the torso, including wall bars, can only increase diastasis and should be excluded. Young mothers can start exercising only 4–6 months after giving birth. During this time, connective tissue structures restore their strength.
According to some authors, up to 87% of patients remain dissatisfied with the results of training programs and require surgical treatment [11]. This is probably due to irreversible damage to the integrity of the tendon bundles of the white line of the abdomen.
Surgery
The goal of all diastasis surgeries is to eliminate the enlarged gap between the rectus abdominis muscles and strengthen the newly formed, thinner linea alba. Open classical or laparoscopic techniques, as well as interventions from mini-approaches, can be used. The results for all techniques are similar, so the choice of operation, as a rule, depends on the individual experience of the surgeon. All techniques can be used for the combination of diastasis recti and umbilical hernia [1][6][8][9].
Robotic surgery is more expensive and does not offer advantages over laparoscopic techniques, so it is not used as widely.
Open methods. Access to the extended linea alba is performed through an incision on the anterior abdominal wall: longitudinal above the midline or transverse below the navel if excess fatty tissue needs to be removed. The “fat apron” is removed to prevent suppuration of exfoliated fiber and improve appearance. The surgeon frees the edges of the internal oblique abdominal muscles from fatty tissue, brings them together using numerous individual or several continuous sutures, and then installs a mesh implant over the formed suture.
The operation is traumatic, after which the patient remains in the clinic for 5–7 days. Some authors report that there are no relapses when using open techniques, others report 4% or more relapses [9]. This operation is performed if it is necessary to remove the “fat apron”, and also if the surgeon does not have the skills to perform laparoscopy. In addition, this technique may be preferable when there is a combination of diastasis recti and an incisional midline hernia.
Laparoscopic techniques. The operation is performed through separate punctures on the abdominal wall. The surgeon and assistant, using special manipulators and a video camera, separate the linea alba from the preperitoneal fatty tissue from the abdominal cavity, and then strengthen it with one continuous or several separate sutures. When the diastasis is eliminated, the posterior surface of the abdominal wall can be further strengthened with a mesh implant. This technique can be used for a combination of diastasis and hernia of the white line of the abdomen. The recurrence rate of diastasis after laparoscopic plastic surgery of the linea alba does not exceed 2% [9]. However, using this technique it is impossible to eliminate the “fat apron” if it exists. This operation is carried out if the surgeon has the necessary skills and the technical capabilities of the medical institution.
Techniques using mini-accesses. This operation combines the positive qualities of open and laparoscopic methods for eliminating diastasis. A 4–5 cm long transverse incision is usually made below the navel at the level of the bikini line or directly above the navel (depending on the extent of the diastasis). Then, a channel is formed in the subcutaneous fatty tissue above the linea alba for the surgeon to work with. Viewing in the canal is usually carried out using a special video camera, as in laparoscopy. The surgeon also approximates the inner edges of the rectus abdominis muscles and then strengthens the anterior abdominal wall with a mesh implant [12]. The recurrence rate using the mini-approach is approximately the same as with open surgery. The technique is used if there are contraindications for laparoscopy (severe adhesive disease in the abdomen after surgery, severe chronic heart failure).
If the clinic has the necessary equipment and a qualified plastic surgeon, each technique can be supplemented with liposuction and liposculpture, in which excess fat is removed from certain areas of the abdomen and thus the relief of subcutaneous fat is formed.
Possible complications after surgery:
- Bleeding with the formation of a hematoma of the surgical wound or in the abdominal cavity. If the bleeding stops on its own, the hematoma does not increase, no blood comes from the wound and the patient feels normal, the hematoma is removed. If the bleeding continues, it must be stopped: remove several stitches and stitch or cauterize the bleeding vessel.
- Seroma of a postoperative wound. This is an accumulation of serous fluid in the thickness of the abdominal wall, namely in the area where the surgeon freed the linea alba from fatty tissue. It manifests itself as swelling and thickening of the subcutaneous fatty tissue. The seroma is removed by a surgeon in the dressing room. If the seroma suppurates, urgent hospitalization is required in the purulent surgery department. This complication is less common during laparoscopy [9].
- Suppuration of the postoperative wound and mesh implant. The operation site turns red and hurts, body temperature rises, chills and sweating appear, especially in the evening. With this complication, it is necessary to remove the pus from the wound and prescribe antibacterial therapy. It is often necessary to remove the mesh implant. It is not known exactly how often surgical wounds fester; according to some data, the complication rate can reach 2% or more [9]. Suppuration occurs due to the addition of infection, especially if there are foci of infection in the body: carious teeth, chronic tonsillitis, chronic inflammatory diseases of the urinary tract (cystitis, pyelonephritis) and female genital organs (salpingitis, endometritis).
- Severe pain in the wound area in the first month after surgery or longer than three months. The patient is concerned if nerve fibers are damaged or compressed during surgery. With such a complication, a second operation may be required: release of the nerve from compressive tissue, removal of the mesh implant, excision of the postoperative scar, removal of the sutures fixing the mesh implant [1][9]. Some authors report that chronic pain syndrome after open surgery can be detected in 17% of patients; laparoscopy can reduce this figure to zero [9].
It is not known exactly how often complications develop after surgery, since in most cases treatment is carried out in private clinics and complications are not included in registries. On average, the incidence of complications is up to 10–15% [9].
Exercises for diastasis after childbirth
Exercise "bridge"
To perform the exercise, you need to lie on the floor and bend your knees (arms straight along the body). As you inhale, lift your pelvis, hold it for a few seconds and lower it as you exhale. Repeat 10-15 times.
Pelvic floor exercises can help strengthen the deep abdominal muscles because all the major muscles automatically contract as a group. These exercises can be performed in the early postpartum period.
Exercise “squatting near a support”
Stand straight next to the wall, pressing your back against it. Next, you should squat to a 90-degree angle, placing a rubber ball between your legs (if you don’t have a ball, you can use a book or a small bottle of water).
Leg raise exercise
Starting position - lying on the floor, on your back, arms extended along the body. One leg is bent at the knee, the other needs to be raised up and straightened, holding it in the air for 3-5 seconds. Repeat the same with the other leg. You need to reach 3-5 sets of 20 repetitions.
How to determine diastasis
If visually in a standing position you do not see significant changes, a simple test will help determine the presence and level of diastasis:
Lie on your back with your legs bent and your feet on the floor. Place one hand on your stomach, placing your fingers on the midline of your navel. Press down lightly with your fingertips and lift your head (shoulders on the ground) as if you were about to begin a crunch exercise.
Feel the area between the rectus abdominis muscles above and below the navel, assess how separated they are. Separation is usually measured by the width of the fingers - for example, one to two or more. If the discrepancy is more than four fingers, then you need to have surgery and exercises will not help.
In other cases, even if there is no diastasis, the following set of exercises will help you find a flat and toned stomach.
Twisting the tailbone in a half-bridge
This seemingly simple exercise helps you learn to engage the necessary muscles and loosen the pelvic area, which is tight and spasmodic in most women.
Lie on your back, bend your knees. Hands on the sides of the body, feet on the floor. Inhale deeply, then exhale slowly, and as you exhale, pull in your stomach. Squeeze your buttocks, lift your pelvis. Bring your tailbone forward and relax several times for 1 minute, then gently lower your pelvis to the floor.
Possible errors: acute angle in the knee joint. Place your feet away from your body.
If you had a natural birth, you can start doing this exercise after a week, but if you had a caesarean section, it is recommended to wait about 8 weeks before exercising.
Classic half bridge
The bridge is a well-known exercise that you may have done before in the gym. However, this one is done a little differently. Lie on your back with your feet shoulder-width apart. Bend your knees, inhale, then exhale, pulling your abs toward your spine.
Then gently push your pelvis up and then lift your hips off the floor. Pause for 2 seconds and then return to the starting position. Repeat up to 10 times.
Table top
The starting position is the same as in the previous exercise. Take the position and tighten your abs. Raise your shins until they are parallel to the floor. Alternately lower the toes of one and the other leg, while the second returns to its original position. Repeat 10-15 times on each leg.
Reduction and separation of the knees
Leave your legs in the previous position. Inhale and tighten your abdominal muscles even more, slowly and smoothly. Hold it and in this position, bring and spread your knees as wide as possible, and then slowly close them.
At the same time, pay attention to the abdominal muscles. Don't let them relax. Repeat 10-15 times.
Towel pull
Lying on your back, cover the top of your shin with a towel and grasp each end. Squeeze your thighs together while pulling firmly on the ends of the towel. Inhale and then exhale, contracting your abs. Then lift your shoulders off the floor.
While holding this position, contract and then relax your abdominal muscles 10-12 times (the number should increase each time).
Pushing a towel
You can add this exercise to your routine 12 to 14 weeks postpartum. Lie on your back with your knees higher than your hips and your shins parallel to the floor. Place a towel on your thighs, grasp the ends and press down on your thighs to create resistance.
Simultaneously lift your head and shoulders, extend one leg and exhale. Switch legs and repeat up to 10 times.
Isometric crunches
Crunches are a common exercise that helps bring your abdominal muscles back together. In this variation, we will lift the head and shoulder blades off the floor and hold for several seconds.
Make sure that your stomach does not form a “house”; to do this, constantly pull your stomach into yourself. Gradually increase holding this position to 30 seconds.
Wall Chair Pose
Stand with your back to the wall at a distance of a small step. Bend your knees to a 90-degree angle, keeping your abs drawn in all the time. You can hold a ball or block between your knees and squeeze it additionally with your thighs. Hold this position for 30 seconds, then return to a standing position.
Breathing exercises for diastasis
Breathing exercises help retrain the diaphragm, or rather, return it to its normal position and functioning. During pregnancy, the growing uterus seems to push the diaphragm up and it loses the ability to return to its normal position. Since the diaphragm forms the upper part of the core muscles, it is important to retrain it and return it to its original position. Here are some good exercises:
- Lying on your back, with a pillow under your buttocks, raised slightly above chest level, you should take short, shallow breaths into your stomach. This exercise should be done for a minute.
- While sitting, you need to put your hands on your chest and take short and shallow breaths for a minute.
The distance between the two abdominal muscles is not the most important aspect. It is much more important that all the abdominal muscles can work together again, providing quality support to the spine.
Belly after childbirth: a guide to action
Breasts and abdomen after childbirth are the number one topic for women who have recently become mothers, because they want to preserve the beauty of the female body for a long time. Today we continue to talk about restoring female forms after pregnancy and the topic of today’s conversation is the belly after childbirth.
Sarvar Kazimovich, thank you for your time, tell us what happens to a woman’s stomach during pregnancy?
If we consider the abdominal area, then the side facing the spine is inextensible. Potentially, the belly can grow in the remaining three directions. During pregnancy, this vector is directed forward. The increase occurs due to the fact that the abdominal wall consists of soft tissue and, accordingly, is stretchable.
From the very beginning of pregnancy, hormones begin to be released into the blood, in particular cortisol, which makes the skin more stretchable. This applies not only to the skin of the abdomen, but also to the integumentary tissues of the mammary glands, which rapidly increase in the first weeks of pregnancy.
What happens to tissues after the birth of a child?
After childbirth, a reverse mechanism is activated aimed at tissue contraction, stimulating the production of collagen and elastin. If a woman during this period additionally engages in physical education, fitness, undergoes massage and cosmetic procedures, then there may be no traces of pregnancy left.
But most often, young mothers have no time to take care of themselves during this period, because they have a newborn in their arms. The body's reserves for restoration, which are activated after childbirth, gradually disappear. Time has passed. Even if the excess fat tissue subsequently disappears, the excess skin is no longer reduced. In addition, often during pregnancy not only the skin, but also the aponeurosis and muscle frame are stretched. Hernias and diastasis (separation of the muscles of the anterior abdominal wall) may form.
It turns out that abdominal exercises are only effective in the first few months after childbirth?
The hormonal boom, which is aimed at restoring the female body, lasts 5-6 months. If during this period a woman actively performs exercises to strengthen the pelvic frame, the anterior abdominal wall, maintain the shape of the mammary gland, uses a contrast shower, special creams, and wears compression underwear, then nature has created all the conditions for everything to be fine.
Evolution has laid down a powerful regenerative mechanism. It only takes a little help for him to return to his previous form.
Let's take a closer look at the case of pregnancy with twins (triplets), when the abdominal distension is especially large.
Even with good skin contractility, twin pregnancy is more likely to cause separation of the muscles of the anterior abdominal wall (diastasis). Sometimes this is accompanied by hernial protrusions. When the abdomen tenses, a ridge appears. A woman can feel it with her hands, pressing on the area of the middle of the abdomen, a “failure” is felt. Upon examination, diastasis or hernia of the anterior abdominal wall is diagnosed, which is already a medical indication for surgical intervention. In such cases, first we perform a hernia repair, restore the aponeurosis, tighten the muscles and at the same time remove excess skin, that is, we restore the aesthetic component of the abdomen.
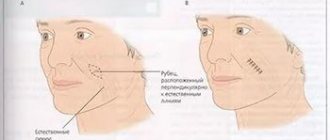
In regular clinics, this is often done through a midline incision, and it looks unsightly, because it leaves a large scar in the visible area. We are trying to hide the scar in the bikini area, which will be covered with underwear and will be invisible even in a bikini.
Next, we combine hernia repair with skin tightening. We rarely use synthetic materials (reinforced with mesh implants). They give a good effect, but for young women planning pregnancy in the future, they are excluded. If necessary, navel surgery and hernia repair in the presence of an umbilical hernia are performed.
What are the most common effects of childbirth on the belly?
The most common consequences: stretch marks, excess skin, diastasis, hernia of the anterior abdominal wall, umbilical hernia. By the way, people often ask about stretch marks (stretch marks), essentially they are burst skin that has not kept up with the growth of the abdomen.
Is mini abdominoplasty applicable after childbirth?
Yes, in some cases you can get by with a mini tummy tuck. Mini abdominoplasty is used when a woman has no problems above the navel and all problems with excess skin are concentrated below the navel.
Is it possible to get by with liposuction of the abdomen after childbirth?
Liposuction works well if there is no excess skin. Those. liposuction directly removes the “layer” of subcutaneous fat. Fortunately, modern women are very active and take care of their health. Therefore, it is easier to remove such excess fat tissue in a fitness club.
How long after giving birth can I contact a plastic surgeon for tummy tuck?
A woman’s hormonal postpartum boom ends by 5-6 months. Accordingly, after 7 months the abdomen will have a reliable, stable shape and a decision can be made on the advisability of surgical correction.
Is it possible to give birth after abdominoplasty?
Yes, you can. We do not use mesh implants for young women, so you can easily become pregnant and give birth after abdominoplasty.
And if we consider this case, everything is fine with the stomach after childbirth, since the woman was actively involved in sports, did abdominal exercises, but the navel stretched and began to protrude a little, can this be corrected?
Yes, sure. The operation is called umbilicoplasty and can be performed under local anesthesia. Often a protruding navel is accompanied by an umbilical hernia. Accordingly, through one cosmetic incision we perform hernia repair and plastic surgery of the protruding navel, fixing it to the deeper layers (often to the aponeurosis). There are skin problems not throughout the abdomen, but around the umbilical area. In this case, skin plastic surgery through mini-accesses above or below the navel is justified.
What recommendations would you give to women on how to properly care for themselves during pregnancy and childbirth, and what to do if problems still remain?
A woman must remember that nature gives her a unique opportunity - powerful genetic recovery mechanisms that operate in the first months after childbirth. We must use this period. If problems remain, almost all consequences can be removed with the help of plastic surgery. Plastic surgery not only provides aesthetic correction, but also solves the pathological component - eliminates diastases, discrepancies, hernias, while not forgetting about beauty.
If a woman has already decided on surgical correction, she must first carefully examine herself, touch, listen to herself - evaluate the areas of discomfort.
After this, you need to come to us for a consultation. There are many options for solving this problem. Everything depends not only on the initial condition of the skin, but also on the condition of the anterior abdominal wall. Consultation with a plastic surgeon at the Mont Blanc clinic is free! Make an appointment by phone. Waiting for you!
Prohibited exercises when diagnosing diastasis after childbirth
Before you start working on eliminating diastasis, you should pay attention to exercises that are strictly prohibited. These include the following types of loads:
- Exercises that require you to lie on your back on a fitness ball.
- Yoga, namely poses that stretch the abdominal muscles.
- Using heavy objects or doing barbell exercises.
- A load that involves being on all fours.
When should you operate?
Most often, diastasis recti goes away on its own within 8 weeks after birth.
If this does not happen, women are usually recommended exercises that help strengthen their abdominal muscles.
The operation is indicated in two cases:
- If diastasis does not disappear within a year or longer.
- If it is combined with a hernia.
In addition to a hernia, diastasis can lead to chronic pain in the lower back and pelvic area, poor posture, and dysfunction of the pelvic floor muscles, which can lead to stress urinary incontinence and pelvic organ prolapse.