13-cis-retinoic acid (13tsRK) as a treatment for ACNE
Information about the structure and function of the sebaceous glands in humans, the hormonal regulation of their function, and the pathogenesis of acne is summarized. The literature on the possible ways in which 13cRK influences the function of the pilosebaceous follicle is analyzed. Information is presented on the clinical effect of 13cRK in severe forms of acne.
Brief information about the structure and function of the sebaceous glands
Sebaceous pilosebaceous follicle
is a complex that includes hair, follicle and sebaceous gland. Each hair follicle is associated with a sebaceous gland, with the exception of the meibomian glands of the eyelid, the thai glands of the preputial sac, the Fordyce glands of the areola of the nipple, the sebaceous glands along the edges of the lip and the mucous membrane of the genital organs, which are not associated with the hair sac and come to the surface of the skin independently. The follicular rudiment is formed at the 8th week of embryonic development by invaginating the epidermal layer deep into the dermis. From the 9th week, the hair growth zone, sebaceous and sweat glands are formed. Starting from the 13-15th week of embryogenesis, the sebaceous glands already function according to the holocrine type. The first hair becomes visible in the 5th-6th month of pregnancy.
Sebaceous gland
consists of terminal sections formed by sebocytes and an excretory duct through which it is connected to the hair canal. In different areas of the skin, the sebaceous glands differ in size. The largest glands (especially in people suffering from acne and seborrhea) are found in the skin of the face and scalp.
Terminal section of the sebaceous gland
formed by several layers of sebocytes. On the basement membrane there are poorly differentiated germ cells capable of proliferation. As they lose connection with the basement membrane, cells differentiate, synthesizing on the smooth membranes of the cytoplasmic reticulum and accumulating lipids in the Golgi zone, which gradually fill the entire cytoplasm. As they approach the center of the end section, sebocytes lose their integrity and turn into lard. Sebum accumulates in the sebaceous hair follicle, where cellular detritus and microorganisms are mixed with it. Then sebum is released onto the surface of the skin and combines with lipids of epidermal nature. The role of sebum in humans is unclear, but it is associated with the barrier function of the skin. Fat consists of 60% triglycerides, which, under the influence of P. acnes hydrolases, are converted into free fatty acids, monoglycerides, lipoglycerides and glycerol. The remainder of the lard (about 40%) consists mainly of wax esters and squalene. The latter is produced exclusively by sebocytes, so the quantitative determination of squalene and its metabolites makes it possible to judge the functional activity of the sebaceous glands. The amount of sebum produced varies individually and depends on gender, age, time of day, and ambient temperature. The function of the glands is also affected by hyperhidrosis, diet, stress, occupational hazards, climate, ultraviolet radiation, etc.
The degree of development and functional activity of the sebaceous glands are, to a certain extent, genetically determined processes. It is known that about 80% of identical twins suffer from seborrhea and acne together. Up to 50% of patients with severe forms of acne have this pathology in their family. Acne develops in everyone who has inherited increased skin elasticity.
Hair canal
is divided into two parts: acro-infundibular (above the confluence of the sebaceous gland duct) and infra-infundibular part (below the confluence). The epithelium and its stratum corneum of the acro-infundibular part are similar to that of the epidermis. The stratum corneum of the infra-infundibular part is less compact; corneocytes are weakly connected to the cells below the layer and are easily removed with sebum.
Sebaceous gland channel
, especially if the gland is large, has the same epithelium and stratum corneum as the lower part of the hair canal.
Sebaceous follicles can be divided into three types. The first type is sebaceous follicles with terminally located small glands (the skin of the eyebrows, the edges of the eyelid, the beards of animals). The second most common type of follicle is characterized by the location of medium-sized sebaceous glands on the side of the hair canal. The third type of pilosebaceous follicle is characterized by a large excretory duct up to 2.5 mm in diameter. These follicles (the hair in them may not always be visible) are found on the face and upper torso. They may contain varying numbers of glands, and within the gland - terminal sections, differ in different lengths of excretory ducts and, in general, represent a large complex that is distinguishable by eye. These follicles are sometimes referred to as “sebaceous follicles.” It is important to note that only type 3 pilosebaceous follicles are affected by acne. Patients with acne have much more type 3 pilosebaceous follicles. Their sizes vary greatly. They are larger on the cheeks and neck and smaller on the back. But on the back they are located, as a rule, in groups of 2-3 complexes. The large excretory ducts of the sebaceous glands of such follicles are usually filled with sebum and cellular debris; P. acnes also colonize here.
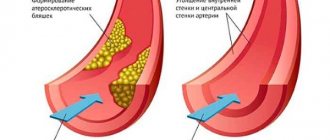
There is evidence that impaired keratinization of the follicular epithelium plays a certain role in the pathogenesis of acne. This applies primarily to the epithelium of the infra-infundibular part of the hair sheath. In patients with acne, the epithelium in this part of the follicle usually has a thick granular and compact stratum corneum. Epithelial cells of the granular layer contain lipid droplets that differ from those of sebocytes and can be considered pathological because they resemble lipid inclusions in psoriasis. The presence of a developed stratum corneum leads to the fact that the keratin mass accumulates in the lumen of the hair canal. And this can lead to the formation of a comedon (a hair follicle filled with “sebaceous filaments”). Sebaceous filaments contain sebum, cellular detritus, epithelial cells and microorganisms. Microcomedones are characterized by thickening of the stratum corneum of the follicular epithelium. The granular layer is usually also thickened, its cells are tightly connected to each other and contain very large keratohyalin granules. Epitheliocytes of deeper layers, unlike the norm, contain lipid inclusions. Such cells are characterized by a reduced content of keratosomes and the appearance of lamellar bodies. The proliferative activity of the follicular epithelium in these cases is usually increased. The described picture is typical for so-called “closed” comedones. With “open” comedones, the epithelium of the acro-infundibular part of the hair sheath is additionally involved in the keratinization process.
Functioning of the sebaceous glands
is a hormonally dependent process. The greatest growth and high functional activity of the sebaceous glands is observed in men during the period of maximum androgenization; castration is accompanied by the reverse development of these structures. The administration of androgens to castrated animals in the presence of tropic pituitary hormones increases sebum production.
Sebocytes
are target cells for testosterone, which regulates lipidogenesis. In sebocytes, the enzyme 5-a-reductase converts testosterone into its active form, dihydrotestosterone, which binds to cellular receptors in the sebocyte nucleus and induces the corresponding transcription processes. There is an assumption that testosterone can regulate the proliferation of sebocytes, but its interaction with T-lymphocytes, which are also capable of controlling the processes of reproduction, remains unclear.
In addition to the testes, the source of testosterone is also the ovaries and adrenal glands. Thyroid hormones, under the influence of which activation of 5-a-reductase is observed, can increase the amount of the biologically active form of testosterone.
In men, acne occurs against the background of high levels of dihydrotestosterone.
In women, the development of acne is accompanied by menstrual irregularities and hirsudism. Increased activity of sebocytes and, as a result, increased sebum production may be due to high activity or high content of cellular testosterone receptors, but the details of this process are not clear. Chu (1995), summarizing the available literature data, comes to the conclusion that the main hormone that regulates the rate of sebum secretion is testosterone. Most other hormones act on sebum production mainly indirectly through testosterone (see table). More detailed information on the issues raised and bibliography can be found in the works of Harms (1990), Sokolov et al. (1988). Factors affecting sebum secretion
| Factor | Effect on the rate of sebum secretion |
| Progesterone | does not affect |
| Adrenal androgens | stimulates in women and castrates |
| ACTH | reduces in women due to its effect on the adrenal glands |
| A growth hormone | does not affect |
| Thyroxine | in rats causes atrophy of the sebaceous glands, acts indirectly through testosterone |
| Topical steroids | inhibit due to antiproliferative effect on sebocytes |
| Antiandrogens | reduces partly due to local action and partly due to inhibition of testosterone production |
Effect of 13cRK on the epidermis and sebaceous glands
As already noted, the epithelium of the ducts and terminal sections of the sebaceous glands is histogenetically related to the epidermis and epithelium of the hair vagina and is their derivative. The effect of 13cRK on the epidermis has been studied in more detail than on sebocytes. Since the reactive properties of cells of the same histogenetic series are similar for many reasons, consideration of literary information on the effect of 13cRK on the epidermis can, by analogy, contribute to understanding the effect of this substance on the morphogenesis of the sebaceous glands.
When administered systemically, 13cRK, bound to transport proteins, is delivered to the skin and accumulates in the epidermis (Siegenthaler et al, 1987). The mechanism of entry of 13cRK into epithelial cells is not clear. The entry of 13tsRK into keratinocytes does not correlate with the level of retinoic acid-binding proteins in the cells, and the accumulation of the substance in the epidermis when applied locally is not dose-dependent. Nevertheless, Saurat (1992), summarizing data on the mechanism of action of retinoic acid, provides a scheme according to which retinol in the body is converted into retinal and into retinoic acid. The latter, through cellular protein, enters the cytoplasm and then, with the participation of a number of receptors, into the nucleus, interacts with the genome with the formation of messenger RNA and specific proteins.
The effect of 13cRK on unchanged skin is accompanied by desquamation and erythema. This indicates changes in both the epidermis and dermis, which require more detailed consideration. According to Breiner et al. (1983), the action of 13cRK leads to hyperplasia of the basal and suprabasal layers of the epidermis, an increase in the number of cells of the spinous layer, deep ingrowth of epidermal ridges and elongation of the dermal papillae (Elias and Williams, 1985). In in vitro experiments using deepithelialized dermis, 13cRK stimulated the proliferation of keratinocytes seeded on the dermal substrate. This, as in in vivo conditions, was accompanied by an increase in the number of epithelial cell layers and signs of suppression of cell differentiation (Ponec et al, 1988). Connor and Lowe (1985) provided evidence that epidermal hyperplasia is a specific and not a toxic effect of 13cRK. Ultrastructurally, epidermal hyperplasia caused by 13cRK is accompanied by disorganization of the stratum corneum, weakening of desmosomal connections, expansion of intercellular spaces with the accumulation of a matrix of average electron density, a decrease in the content of tonofibrils in cells and the deposition of glycogen (Schultz-Erendurg, Orfanos, 1981). According to Tammi et al. (1989), hyaluronic acid derivatives can accumulate in widened intercellular spaces. It is possible that the resulting matrix includes glycoproteins and glycolipids, since 13cRK controls their synthesis and affects the stability of cell membranes. According to Afanasyev and Volkov (1989), retinoic acid and its derivatives stimulate the processes of proliferation of the epidermis and hair sheaths, leading to the accumulation of poorly differentiated cells in the population. At the same time, keratinization processes decrease, the stratum corneum becomes thinner, and hair falls out.
Tsambaos and Orfanos (1981) analyzed the literature data on the specific effects of 13tsRK on epithelial proliferation and differentiation and came to the conclusion that they may be associated with the ability of 13tsRK to activate RNA polymerase, DNA and RNA synthesis. There are indications of the ability of retinoic acid to control the synthesis of certain types of keratins (Wolf, 1984). Petkovich et al. (1987) discovered a cellular receptor specific for retinoic acid in keratinocytes, which corresponds to the HK1R gene. The ability of 13cRK to interact with receptors of the g-22 locus of the 17th chromosome was shown in acute promyelocytic leukemia cells. It is significant that genes responsible for morphogenesis processes are localized in the g-21 and g-22 loci (Mattei et al, 1988). A consequence of the influence of 13cRK on transcription and translation may be a change in the synthesis of glycosylated molecules and the processes of cell-cell interactions and proliferation. There are reports of the ability of 13tsRK to influence the proliferation of epidermal cells by changing the activity of Ca++-dependent protein kinase C and the binding ability of receptors for epidermal growth factor (Peck et al, 1988).
By changing vascular permeability, promoting the formation of accumulations of granulocytes, monocytes, macrophages, lymphocytes, retinoids are able to influence the structural components of the dermis. This, in turn, affects the processes of proliferation and differentiation of integumentary epithelial cells (Tsamboas, Orfanos, 1981). 13tsRK also has similar properties. Thus, co-cultivation of epidermocytes and fibroblasts in a medium with 13cRK led to the suppression of epithelial proliferation. If fibroblasts were inactivated, the epithelial cells proliferated (Sanquer et al, 1988). In vitro, 13tsRK stimulates the attachment of monocytes to the endothelium (Barkley et al., 1987); in the dermis of laboratory rodents, it increases the content and phagocytic activity of macrophages (Afanasyev et al., 1983, 1986). According to our information (Nozdrin, Volkov, 1995), retinoids can be considered as indirect regulators of monocyte/macrophage functions. Shcherbakov (1990), summarizing a fairly wide range of works, comes to the conclusion that macrophages, including Langerhans cells, have a growth-stimulating function in relation to keratinocytes. The effect is achieved due to the release of interleukins 1 and 6 by macrophages, which activate the proliferation of skin epithelial cells.
Hypervitaminosis A is accompanied by a decrease in the content of T-helper cells in the lymph nodes of mice (Carmam et al, 1989). In humans, 13cRK is capable of changing the number and functional activity of NK cells and the ratio of helper-suppressor forms of lymphocytes (Shuttleworth et al, 1988). 13cRK in a mixed culture of lymphocytes is capable of dose-dependently stimulating the formation of T-killer cells. T-lymphocytes of the spleen of mice can transfer the ability of 13cRK to activate the proliferation of the epidermis (Afanasyev, Volkov, 1989).
There are only a few reports on the effect of 13tsRK on unchanged sebaceous glands. Thus, in an experiment on hamsters it was found that under the influence of 13cPK the size of the sebaceous glands of the lateral organ decreases and their production of sebum decreases (Gomez, 1981). A relatively detailed study of the effect of 13cPK on the sebaceous glands was carried out when examining the skin of male patients with various forms of acne (Landthaler et al, 1981). It has been established that under the influence of 13cRK the size of the sebaceous glands decreases, the ratio of differentiated and undifferentiated sebocytes changes towards an increase in the pool of precursor cells and a decrease in thermally differentiated cells that turn into detritus. In our experiments, 13cRK dose-dependently reduced the size of the sebaceous glands of the skin, increased the proliferative activity of sebocytes, and decreased the content of highly differentiated cells in the population capable of turning into sebum.
Of undoubted interest are the studies of Zonboulis et al. (1991, 1992), carried out on cells from a surviving culture of human sebocytes. In these experiments, 13cRK changed the proliferation and differentiation of sebocytes, as well as the synthesis of total lipids, cholesterol, triglycerides, and the expression of keratins.
Effect of 13tsRK on ACNE
Acne
is a multifactorial process based on the pathology of the pilosebaceous follicle. The most common form of acne is juvenile acne. This form of the disease is characterized by seborrhea with typical changes in the pilosebaceous follicles (comedones, papules, pustules, and often scars). The lesions are localized mainly on the face, back, and chest. The onset of the disease is associated with the period of formation of sexual function. In a mild form, the disease is found in 100% of boys and 95% of girls, in a moderate form - in 98% of boys and 80% of girls. Severe forms of acne occur in 19.5% of boys and 18.2% of girls.
The pathogenesis of acne is based on:
- genetic background;
- increased sebum production due to stimulation of terminal differentiation of sebocytes by androgens;
- difficulty in the outflow of sebum due to keratinization of the epithelium and narrowing of the mouth of the excretory ducts;
- P. acnes infection.
The role of P. acnes in the pathogenesis of acne remains unclear.
Harms, (1990), summarizing the literature, offers several versions of such participation:
- P. acnes, releasing a chemotactic factor for polymorphonuclear leukocytes, induces inflammation;
- P. acnes activates the function of polymorphonuclear leukocytes, which damage the wall of the hair follicle, promote the release of triglycerides into the dermis and provoke inflammation;
- P. acnes activates complement, which is also activated by the antigen-antibody reaction; P. acnes is well known to enhance antibody production;
- polymorphonuclear leukocytes, under the influence of chemotactic factors, secrete lysosomal enzymes that destroy the gland wall; inflammation develops in response to the entry of sebum, free fatty acids, hair components, cellular debris and P. acnes into the dermis.
Relatively many works have been devoted to studying the influence of 13cRK on the course of acne, so only the most complete and well-known of them will be presented here. One of the first reports on this topic was made by Resk et al. (1979). The authors treated 13cRK in 8 men and 6 women with advanced and antibiotic-resistant forms of acne. The substance was prescribed at 0.5 - 1 mg/kg/day for 4 months. In 13 patients there was a complete cure, in 1 patient about 75% of the lesions disappeared. The administration of 13cRK to 14 men aged 16 to 31 years with severe forms of acne at 0.1 - 1 mg/kg/day had a therapeutic effect in more than 90% of cases. The effect increased with the dose and duration of administration and was maximum with a 3-month course of treatment at 1 mg/kg/day. The therapeutic effect was accompanied by a decrease in skin inflammation; lesions were replaced by scars (Farrel et al, 1980). Similar data are provided in the studies of Jones et al. (1981) - 10 observations, Ott and Geiger (1982) - 15 observations. Plewig et al. (1981) presented the results of a study of 60 patients who suffered from various forms of acne that were resistant to traditional treatments. Patients received 13cRK at a dose of 0.5 - 2 mg/kg/day for 12 - 24 weeks. The substance exhibited a clear therapeutic effect: the secretion of glands decreased, ductal keratinization was normalized, the separation of sebum was facilitated, and the inflammatory reaction subsided. According to Jones et al. (1981), 13cRK at a dose of 0.1 - 1 mg/kg/day for 16 weeks had a therapeutic effect in 22 patients with acne resistant to antibiotics. Similar results with the use of both 13cPK and isotretinoin (IT), an oral dosage form of 13cPK from Roche, are reported by Strauss et al. (1981) and Landthaler et al. (1981). A comparative study of the treatment of various forms of acne with 13tsPK and erythromycin, conducted on 77 patients by Jones et al. (1984), showed that 13tsPK is the preferred agent in terms of effectiveness and that the antibiotic does not improve the therapeutic effect of 13tsPK. Mack et al. (1984) published the results of treatment with IT (0.05 - 0.2 mg/kg/day) for 20 weeks in 174 patients of both sexes aged 14 to 24 years with papular-pustular forms of acne. The positive effect of treatment was achieved in 84% of patients, accompanied by a decrease in sebum production and the reverse development of foci of inflammation.
Reports of the effective use of drugs with 13cRK for the treatment of severe forms of acne were made by Meigel et al. (1983) - 198 patients, Plewig et al. (1981) - 64 patients, Goulden et al. (1995) - 200 patients. Verschocre and Schaefer (1991), Shalita (1992), Sendagorta (1992) reported successful topical use of soft dosage forms of 13tsPK for mild to moderate acne. Schmidt et al. (1983) reported that in 15 patients receiving 13cRK for conglobate and cystic forms of acne, a positive clinical effect was accompanied by a decrease in sebum secretion. A detailed study of the sebaceous formation process conducted by Blake et al. (1988) in acne patients who received IT showed the following. During the first 4 weeks from the start of treatment, there is a significant decrease in the level of sebum excretion. By the end of the course, this indicator was reduced compared to the initial level by 4-5 times and remained reduced until 4 years after discontinuation of the drug. Moreover, more than half of the patients did not require repeated courses of treatment. According to Shalita (1984), the therapeutic effect of 13cRK is achieved due to the concentration of the substance in the sebaceous glands. In this case, there is a delay in the differentiation of sebocytes and a decrease in sebum production. The anti-inflammatory effect of the drug may be due to its immunomodulatory properties. Layton et al. (1993), summarizing ten years of experience in the use of IT in the treatment of 387 patients with acne, come to the conclusion that in order to achieve a sustainable effect, it is necessary to take into account not only the daily, but also the course dose of the drug. A stable (5-10 years) positive effect without the use of antibiotics and without repeated courses of IT in 61% of patients was observed at a daily dose of 1 mg/kg and a total dose exceeding 120 mg/kg.
Side effects of the use of 13cRK (cheilitis, changes in keratinization, dermatitis, nosebleeds, conjunctivitis) were already noted in the first reports. Peck et al. (1981) analyzed the incidence of complications in 26 patients who received 13cRK at 0.1 - 1 mg/kg/day from 2 to 6 months. All patients developed cheilitis, 20 - changes in the epithelium of the eyeball, 16 - dermatitis, 15 - xerosis, 13 - runny nose and nosebleeds, 4 - hair loss, 4 men - urethritis, 3 - arthralgia , skin itching. With long-term use in high doses, 13cRK can inhibit the function of the meibomian glands, cause lacrimation, blepharitis, conjunctivitis, keratitis, and changes in dark adaptation. At a dose of 2 mg/kg/day or more, 13cRK provokes hyperostosis of the spine and calcaneus. There are reports that the use of 13cRK can have a hepatotoxic effect, inhibit the production of androgens, cause hypercholesterolemia, neutropenia and mild anemia. It should be noted that the listed complications are mostly reversible and regress after discontinuation of the drug. The most alarming effect of 13tsRK use is teratogenicity. 13tsRK, when administered to pregnant women, can cause disruption of the formation of the facial skeleton, malformations of the heart and large vessels, anomalies of the central nervous system, retina, and optic nerve in the fetus (Rothman, Pochi, 1988). In this regard, the main condition for prescribing the drug in women of childbearing age is the use of contraceptives during treatment and up to 2 years after discontinuation of the drug. Pregnancies that occur during the use of 13tsRK must be terminated (Leyden, 1988). Straus et al. (1988) appealed to patients to strictly adhere to the indications for use of the drug and to protect themselves from pregnancy (13cPK does not have a toxic effect on spermatogenesis in therapeutic doses). Failure to comply with these conditions may lead to an increase in the birth rate of children with congenital developmental anomalies and, ultimately, to a ban on the use of the substance as harmful to humans. IT has similar side effects (Orfanos, 1985). There are reports that treatment of acne with drugs containing 13 tsRK may be accompanied by staphylococcal pyoderma (up to 4% of all treated), which is relieved by local use of antibiotics, multiple purulent granuloma-like lesions of the sebaceous glands with ulcerations, necrosis and signs of general intoxication. Such conditions developed in patients with a marked decrease in the content of T-lymphocytes in the blood (Driesch et al, 1986).
In connection with possible complications, the question arises about the dosage and duration of treatment. According to Plewig et al. (1981), who analyzed 136 observations of acne conglobate, the therapeutic effect increases with increasing doses of IT. However, with a progressive increase in the dose of the drug, the positive effect increases by no more than 2 times. Moreover, the substance at a dose of 0.2 mg/kg/day causes fewer complications than a dose of 1 mg/kg/day. Similar results were obtained in the works of Farrel et al. (1980) and Jones et al. (1980). In these studies, the drug was given for 12 weeks. The therapeutic effect appeared from 2-3 weeks, continued to increase for 3 weeks and persisted up to 8 weeks after discontinuation of the drug. According to Wokalek et al. (1984), after a 12-week course of treatment in most patients, remission lasts at least 3 months.
There are reports that 13tsRK can also be effective in the treatment of fungal mycosis (cutaneous T-cell lymphoma), pustular psoriasis, scleroderma, hidradenitis, seborrhea, rosacea.
All these data are taken into account by Roche in the “Instructions for the use of Roaccutane” (1990). The authors note that Roaccutane reduces seborrhea, has an anti-inflammatory effect, reduces hyperkeratosis of the orifices of the glands, inhibits the growth of P. acnes, and reduces the size of the sebaceous glands. The drug is indicated for severe forms of acne that do not respond to conventional treatment methods. The drug is effective in 80-90% of patients. Its main disadvantage is teratogenicity. The duration of treatment is 16-24 weeks at a dose of 0.1 -1 mg/kg/day. Side effects are dose-dependent, reversible and disappear after discontinuation of the drug. Cheilitis and dermatitis can be reduced by using a fat base, steroid ointments, and erythromycin. Blepharitis and conjunctivitis - with ophthalmic antimicrobial agents (contact lenses should be replaced with glasses). If headaches, myalgia and arthralgia occur, analgesics are prescribed, the dose is reduced or the drug is discontinued. The dose of roaccutane is reduced or even canceled if the content of triglycerides, cholesterol, lipoproteins, transaminases, uric acid, etc. in the blood increases significantly (2 times). The drug is not prescribed to women planning pregnancy, pregnant women, nursing mothers, patients with hypervitaminosis A, hepatic and renal failure, hyperlipidemia. Roaccutane is not prescribed in combination with vitamin A and tetracycline.
Thus, the effect of 13cRK on the epidermis is accompanied by increased proliferation of keratinocytes, leading to hyperplasia of the epidermis, accumulation of low-ploidy, poorly differentiated cells in the population, a decrease in the strength of intercellular connections, a decrease in keratinization processes, and easier desquamation of corneocytes. The effect can be direct or indirect through dermal cells. The effect of this substance on the morphogenesis of keratinocyte and sebocyte populations is fundamentally similar. It is expressed in increased proliferation and a decrease in the degree of cell differentiation. A reflection of this process is a decrease in sebaceous formation and inhibition of ductal keratinization. 13cRK can have a sustained therapeutic effect on acne of varying severity. The action of the substance is accompanied by side effects, the most significant of which is teratogenicity. The optimal doses of the drug, depending on the severity of the disease, are 0.2 -1 mg/kg/day, and the duration of treatment is up to 12 weeks. Prescribing 13cRK (IT, roaccutane, accutane, etc.) to women of childbearing age requires the use of contraceptives both during treatment and for a long time (up to 2 years) after discontinuation of the drug; Any pregnancy that occurs must be terminated for medical reasons. Previous or planned pregnancy is an absolute contraindication for the use of retinoids.
IN AND. Nozdrin, Yu.T. Volkov
What substances are called retinoids? Their use in the practice of a cosmetologist.
Retinoids are a chemically related class of compounds to retinol (vitamin A), its biological and structural synthetic derivatives; they differ from the isoprene structure of natural vitamin A, but act in a similar way; through the activation of nuclear retinoic receptors they regulate the processes of proliferation, differentiation and intercellular communication of cells.
Retinoids are either topical (for external use) or systemic (for oral use).
For external and systemic use, retinoids:
- have anticomedogenic, sebostatic, anti-inflammatory, kerato- and immunomodulatory effects;
- influence the development and division of epithelial cells;
- activate regeneration processes in the skin;
- normalize follicular hyperkeratosis;
- stimulate the creation of new blood vessels and the production of connective tissue fibers of the dermis;
- suppress the activity of bacteria;
- reduce sebum production;
- increase the production of mucopolysaccharides and glycosaminoglycans.
They reduce the likelihood of skin cancer, some forms are even used in oncology to treat certain types of cancer, reduce pigmentation (post-acne, age spots) and show antioxidant activity. Retinoids have been widely used in dermatological practice since 1963, when the effectiveness of retinoic acid for acne was proven, and are also used to treat psoriasis.
In cosmetology the following are used:
- to reduce the manifestations of photoaging, hyperkeratosis, hyperpigmentation;
- regulation of the sebaceous glands – acne therapy;
- as an anti-aging component, stimulate cell renewal, reduce the area and number of wrinkles. They also have an effect on fibroblasts, triggering the production of collagen, elastin and hyaluronic acid;
Retinoids are divided into three generations (in some publications you can find four), each with stronger and weaker forms.
First generation: retinoic acid derivatives – vitamin A (retinol acetate, retinol palmitate), retinal (retinaldehyde), tretinoin (trans-retinoic acid, ATRA), isotretinoin (13-cis-retinoic acid), alitretinoin (9-cis-retinoic acid ).
They are natural retinoids synthesized in the human body; all subsequent generations are synthetic, obtained in laboratory conditions.
Retinyl palmitate → Retinol → Retinaldehyde/retinal → Retinoic acid
The closer the retinoid is to retinoic acid in this chain, the more effectively it affects the skin, but the higher the likelihood of side effects such as irritation, peeling or dryness.
Used in cosmetics:
Retinyl palmitate – moisturizes and tightens the skin, stimulates collagen synthesis.
Retinaldehyde/retinal - fights obvious signs of aging, antibacterial effect (helps with acne). Suitable for sensitive skin.
Retinoic acid is an effective ingredient for wrinkles and acne. Retinoic acid products are available by prescription.
The concentration in homemade anti-aging creams is usually no more than 0.1%. In more serious medicinal drugs - from 0.4% to 1%. The higher the concentration, the stronger the effect and the higher the risk of irritation.
For the treatment of severe forms of acne and acne that are reactive to systemic antimicrobial agents, first generation systemic retinoids - isotretinoin - . Oral administration of drugs containing 13-cis-retinoic acid is prescribed. It has anti-inflammatory, keratolytic and antiseborrheic effects, inhibits terminal differentiation of keratinocytes, and stimulates regeneration processes.
Second generation: etretinate and its metabolite acitretin. Used as systemic drugs for the treatment of psoriasis and dermatoses.
Acitretin is a synthetic aromatic analogue of retinoic acid. For psoriasis and keratinization disorders, the drug normalizes the processes of proliferation, differentiation and keratinization of epidermal cells.
Third generation (arotenoids): adapalene, bexarotene, tazarotene.
In some publications, adapalene is classified as the fourth generation. It is a naphthoic acid derivative that has the properties of vitamin A, but differs in chemical composition from all generations of retinoids. Found only in pharmaceutical products. Adapalene is usually prescribed for acne, but it also works as an anti-aging ingredient.
Tazarotene is prescribed for psoriasis and is not sold in Russia.
Tretinoin, isotretinoin, bexarotene and alitretinoin are also used in oncological practice.
All synthetic retinoids, from the second to fourth generation, are medicinal substances, and they are not allowed in cosmetics.
For training issues: Lyudmila; +79219015105; email Consultation on medications: Oksana, +79119952960; e-mail We will be glad to see you at the address: Ordinarnaya street, 21, St. Petersburg.
Sources: https://flacon-magazine.com/, https://www.make-and-up.com/, https://www.bsmu.by/, https://www.donttouchmyface.co/, https://www.spletnik.ru/, https://www.isclinical.ru/, https://www.mediasphera.ru/, https://kiai.com.ua/
What is retinol?
Find out if you should add retinol to your skin care routine!
Basic moments
- Retinol is one of the most powerful and popular anti-aging cosmetic ingredients used to reduce visible wrinkles, fine lines and hyperpigmentation.
- It also helps reduce the appearance of acne by stimulating cellular turnover.
Retinol is a retinoid, a form of vitamin A, and is the gold standard for reducing the signs of skin aging. It can accelerate cellular turnover and reduce the appearance of wrinkles, fine lines and age spots for firmer, smoother and more even-looking skin. Retinol may also help reduce the appearance of acne by preventing clogged pores.
Why use retinol?
Skin aging occurs for a number of reasons, from environmental factors to stress and natural aging. As the skin ages, cellular turnover and collagen production slow down. Visible signs of skin aging (hyperpigmentation, fine lines, wrinkles, etc.) occur as a result of our skin's natural defense mechanisms and due to slower cell turnover and skin repair. Retinol is an excellent choice for correcting premature aging because it accelerates skin turnover to reduce the appearance of signs of aging.
How does retinol work on the skin?
Retinol stimulates skin cell renewal. Thanks to this, the skin becomes smoother. In order to tolerate retinol well, the skin needs to accumulate so-called “retinoid receptors”. These receptors are proteins found naturally in the skin, and they help retinol do its job. The skin can produce retinoid receptors through controlled exposure, so it is often recommended to start with products containing minimal amounts of retinol and gradually increase the concentration.
Types of retinol
Retinol belongs to a family called retinoids. These are forms of vitamin A that help increase cellular turnover, accelerate skin renewal, effectively evening out skin tone and correcting age-related changes.
Retinoids have the strongest effect on collagen! They work in two ways: they help reduce collagen breakdown from sun exposure and stimulate the production of new collagen.
- Retinoic acid
is a type of retinoid that is available by prescription only in forms such as isotretinoin and tretinoin, but has the greatest potential for skin irritation. - Retinol
is the strongest retinoid available over the counter. Although highly effective, retinol is 20% weaker than retinoic acid and is slowly converted into retinoic acid in the skin. This also means there is less skin irritation than with retinoic acid. - Retinyl palmitate
,
retinyl propionate
, and
retinyl acetate
are the lightest retinoids, also known as retinol esters. They take longer to convert into retinoic acid and carry minimal risk of skin irritation. - Microencapsulated retinol
. Some forms of retinol are microencapsulated, which helps stabilize the retinol for maximum effectiveness. Microencapsulated retinol also creates an invisible shield on the skin's surface to help minimize moisture loss, which is critical to reducing the appearance of wrinkles and fine lines.
How to use retinol
- Start using retinol gradually: slowly increasing your skin's resistance helps reduce the risk of irritation. Start using it once every week, then every other day, and then move on to daily use.
- Use retinol at night to avoid skin irritation from sun exposure.
- Always use sunscreen throughout the day to protect your skin from sun exposure.
- Avoid other exfoliants unless they are intended for use with retinol.
- Monitor your skin with a cosmetologist while using products with retinol.
- Avoid retinol if you are pregnant or breastfeeding.
Does retinol cause flaking, inflammation or redness?
It can take up to several weeks for your skin to adapt to retinol. At the same time, you may experience flaking and minor inflammation, as well as other forms of sensitivity. This is normal and should stop when your skin accumulates retinoid receptors. Some people call this a "cleansing" period, but in reality your skin is building up its receptors through controlled exposure.
Does Retinol Cause Pigment Spots?
Retinol does not cause age spots (hyperpigmentation); in addition, it is used to lighten them. However, retinol makes skin more sensitive to the sun, so if you have retinol in your routine, you should use sunscreen and reapply it frequently throughout the day. Any sun damage can reverse your progress and increase the appearance of age spots and other signs of skin aging.